
Do Not Be Deceived! Medicare For All is Socialized Medicine, and the Democrats' Socialist Bill has 123 Cosponsors- Americans must identify and vote against Medicare For All supporters. https://t.co/4A0aUyXDEz via @kksheld @janeorient @NBSaphierMD @DrKellyVictory @SurgeryCenterOK
— Kris Held,MD (@kksheld) October 24, 2018
Could "Medicare for All" Plans exacerbate this problem with its plans to reduce reimbursements to health care providers? Doctor Shortages Explode Thanks To ObamaCare — Who Could Have Predicted That? https://t.co/NEQJdBghQC via @IBDeditorials
— Greg Karnes (@realGregKarnes) August 21, 2018
ICYMI: These states wanted #MedicareForAll — until they saw the price tag: https://t.co/TLbla4ImzY @JaredWalczak @dcexaminer pic.twitter.com/Vg7Fq0b9Kg
— Tax Foundation (@taxfoundation) August 6, 2018
July 30, 2018
Obamacare Coverage Map as of 7-19-17
March 23, 2017
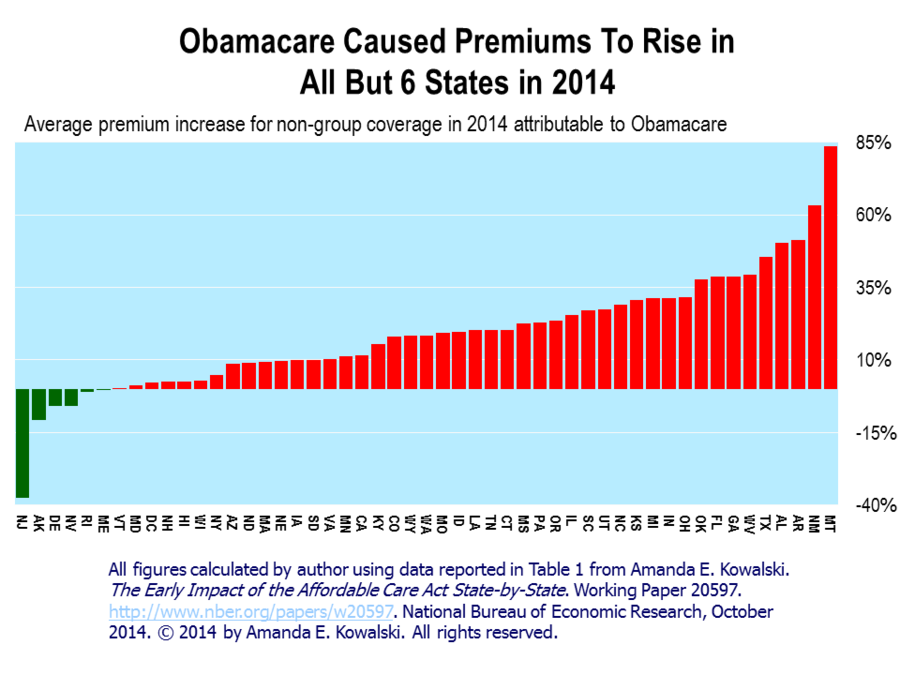
New Analysis: Obamacare Regulations Drove Up Premium Costs by Up to 68%
January 3, 2017
Judge Blocks Obamacare’s Abortion, Sex Change Mandates
HHS interpretation exceeds authority, 'likely violates' religious liberty
February 11, 2016
The Obama Administration’s Design for Imposing More Health Care Mandates (From Edmund F. Haislmaier – The Heritage Foundation)
The Department of Health and Human Services’ Office for Civil Rights has proposed a rule that, if adopted, would dramatically expand federal regulatory power over private health plans and medical providers. The proposed rule would implement section 1557 of the Affordable Care Act (prohibiting discrimination in health programs “receiving federal financial assistance”) in a manner that reinterprets anti-discrimination statutes from ensuring that individuals are not denied access to whatever benefits a plan might provide into legal requirements that plans provide specified benefits. Thus, determinations of the medical “necessity” or “appropriateness” of coverage and treatments would be subordinated to determinations by federal regulators or judges of prohibited “discrimination.” Their decisions would effectively impose new health insurance benefit mandates and, under the rule’s broadly defined scope, those mandates would be imposed not only on Medicare and Medicaid but also on unsubsidized individual and employer plans covering another 164 million Americans.

November 4, 2015
Obamacare Is Dead (From National Review – Kevin D. Williamson)
It doesn’t work because it couldn’t work.
September 9, 2015
The Legalization Of Marijuana In Colorado – The Impact
The most recent study on Colorado’s legalization of dope smoking paints a pretty dim picture for public safety in Colorado
August 24, 2015
Electronic Health Records - A Physician’s View (From National Center for Policy Analysis - Lawrence N. Pivnick)
Electronic Health Records are not yet ready for widespread utilization. They should only be adopted in the normal course of business on their own merits, not under duress. Their full potential will only be realized when they prove useful to the doctor/patient interaction, not otherwise. They should not be foisted upon an unwilling medical profession and its patients for ulterior motives, before proper testing and proof of safety and reliability. At the moment, they are simply another government power grab; a solution in search of a problem.
May 18, 2015
Fifty Changes to ObamaCare … So Far
By our count at the Galen Institute, more than 50 significant changes have been made to the Patient Protection and Affordable Care Act , at least 31 that the Obama administration has made unilaterally, 17 that Congress has passed and the president has signed, and two by the Supreme Court.
March 30, 2015
King v. Burwell: A Loss of Subsidy Does Not Mean a Loss of Coverage
An important distinction is getting lost in commentary on the possible effects of a Supreme Court decision in the case of King v. Burwell. It is the distinction between how the Court’s ruling would affect “insurance subsidies” versus how it would affect “insurance coverage.” Should the Supreme Court’s eventual ruling in King v. Burwell result in people losing insurance subsidies, the affected individuals will have options for maintaining their coverage or choosing replacement coverage. Congress can also reinforce that through oversight hearings, appropriations, or legislation. Of course, some might still not be able to afford the unsubsidized premium even if they switched to a less expensive plan. As a first step to help them, Congress can contribute to bringing premiums back down by exempting individuals, employers, and plans from the costly benefit mandates and age-rating rules imposed by the ACA. That would allow for a rational market to form and thus provide a clearer understanding of the need for assistance.
Adobe Acrobat document [106.6 KB]
March 20, 2015
2015 ACA-Exchange-Premiums Update: Premiums Still Rising
Health care premiums are continuing to rise in 2015, and measuring changes in premiums is an important element in understanding the impact of the Affordable Care Act. Exchange-plan pricing in 2015 generally shows reductions in premiums for the expensive plans that few people purchased accompanied by increases in premiums for the lower-cost plans favored by the majority of enrollees. Thus, the real-world effect for most exchange consumers is that the prices they pay further increased in 2015, though not as dramatically as they did in 2014.
Adobe Acrobat document [115.6 KB]
February 27, 2015
King v. Burwell: An Opportunity for Congress and the States to Clear Away Obamacare’s Failed Policies
Congress and the states should seize the opportunity and clear the way for patient-centered, market-based reforms to take root in the states. Congress should devolve the regulatory authority over insurance back to the states. In anticipation of such an exemption, states should use their authority now to put in place their own policies governing insurance. Congress should not preserve the flawed Affordable Care Act (ACA) subsidy scheme and states should not adopt state exchanges. Instead, congress should exempt individuals, employers, and insurance plans in states that have no state exchange from the ACA’s costly rules, regulations, and mandates.
Adobe Acrobat document [121.3 KB]
February 23, 2015
Impact of King v. Burwell: Obamacare’s Key Design Flaws
Many of the Affordable Care Act’s (ACA) key components are complicated, confusing, and disruptive. The complexity and cascade of adverse effects are the inescapable byproducts of major flaws in the legislation’s basic design. The first flaw is its overly generous subsidies. The second design flaw is a complex tax credit design. Another flaw is the blanket prohibition on pre-existing condition exclusions, which ignored the previous approach which was working well. The fourth flaw is the rating rules that increase premiums, and the final major flaw is the costly and prescriptive benefit mandates. The complexity and adverse effects of the ACA’s key provisions have already increased costs and dislocated millions from coverage. Thus, it is the ACA’s fundamental design flaws—not how the Supreme Court eventually rules in the King case—that are the ultimate source of disruption and will continue to plague the law’s implementation.
Adobe Acrobat document [113.4 KB]
February 23, 2015
Eight Groups Harmed by Obamacare's Flawed Policies
While King v. Burwell is currently in the spotlight, in the end, the Affordable Care Act (ACA) and its flawed policies are at the root of the problems plaguing this law and are responsible for its harmful effects. Taxpayers will be harmed because, despite increasing debt, the ACA creates a new entitlement program and expands the broken Medicaid. Workers are harmed, because employers are cutting employee hours so they fall below the 30 hour threshold. Additionally, faith-based employers are being required to comply with policies they may not agree with. The ACA exacerbates the worst features of our health care system by doubling down on the third-party payment arrangement that compromises the independence and integrity of the medical profession, and thus it harms doctors. Finally, the ACA harms the uninsured. The Congressional Budget Office (CBO) estimates that 4 million individuals will face the mandate penalty, totaling $4 billion, in 2016.
Adobe Acrobat document [109.4 KB]
January 29, 2015
Q3 2014 Health Insurance Enrollment: Employer Coverage Continues to Decline, Medicaid Keeps Growing
Third quarter 2014 health insurance enrollment data show continuation of two trends during the first and second quarters—increasing Medicaid enrollment and declining enrollment in employer plans. However, while individual-market enrollment increased substantially in both the first and second quarters, it declined by 357,000 during the third quarter. The net result was 160,000 fewer Americans with health insurance. For the first nine months of 2014, individual-market enrollment grew by 5.83 million, but 4.93 million individuals lost employer coverage—offsetting 85 percent of the individual-market gain. Thus, the net increase in private health insurance for 2014 is so far 893,000 individuals. During the same period, Medicaid enrollment grew by almost 7.49 million. Taken together, the number of Americans with health insurance increased by 8.38 million during the first nine months of 2014, but growth in Medicaid accounted for 89 percent of that gain.
Adobe Acrobat document [171.4 KB]
January 7, 2015
46 Changes to ObamaCare … So Far
By our count at the Galen Institute, more than 46 significant changes already have been made to the Patient Protection and Affordable Care Act: at least 28 that President Obama has made unilaterally, 16 that Congress has passed and the president has signed, and two by the Supreme Court.
Adobe Acrobat document [1.3 MB]
December 9, 2014
Restoring Balance to Federal Health Spending
Coming to agreements on some provisions of health reform early will set the stage for a productive 114th Congress. It can also create a positive atmosphere for the more significant challenges to come; priorities such as SGR and—even further out—a social security disability insurance solution. In preparation for next year, health care spending will be a continued concern. In setting fiscal priorities for health care, Congress should start with small reforms to the ACA that have the potential for real savings.
Adobe Acrobat document [183.8 KB]
December 9, 2014
Watch: GOP Lawmaker Chokes Up as She Describes Her Tragic, Personal Involvement With Obamacare
December 04, 2014
Power to the People: Repealing and Replacing Obamacare with Patient Power
Obamacare is based on central planning, coercive mandates prescribing from the top down exactly what health insurance everyone must buy. Such central planning naturally involves banning many existing health insurance policies people previously had, liked, and were promised they could keep. The patient power replacement for Obamacare is based on unrestricted individual consumer choice in a competitive marketplace. Voters will wildly and widely applaud replacing Obamacare with patient power.
Adobe Acrobat document [90.4 KB]
November 13, 2014
14 Ways ObamaCare Is Still a Big Mess – That You Won’t Learn from the Liberal Website Vox
ObamaCare is becoming an even bigger mess than it was during the first enrollment period. The program has caused a multitude of problems as the exchanges head into the second open enrollment. Among them increased premiums, poor quality plans, high exchange “dropout rates,” and a shift toward part-time labor. And so much for reducing the deficit! Fewer hours worked, of course, means fewer taxes paid. With over 6 million insurance cancelations last year alone, the fallout of ObamaCare has been worse for America than its critics imagined.
Adobe Acrobat document [1.9 MB]
Caught on Camera: Obamacare Architect Admits Deceiving Americans to Pass Law - “Lack of transparency is a huge political advantage,” says the MIT economist who helped write Obamacare. “And basically, call it the stupidity of the American voter or whatever, but basically that was really, really critical for the thing to pass.” (Barry Soetoro & his crew are dirty, dirty, dirty !!)
November 10, 2104

October 31, 2014
Health Care Providers are Opting-Out of Obamacare Exchange Plans
Health care providers face many obligations and restrictions as a result of the Affordable Care Act, as do insurers. Because of pressure placed on insurance companies to keep cost of exchange plans unrealistically low, providers are reimbursed at unsustainable rates. Reduction in payment rates has caused many physicians and hospitals to decline insurance plans issued through the exchanges, thereby negating the intended effect of providing individuals with affordable care by virtue of eliminating access to care. A market where not only hospitals and physicians are opting-out of exchanges plans, but individuals and families are opting-out as well results. The stated goals of the law fly in the face of the actual results that it produces.
Adobe Acrobat document [200.8 KB]
October 22, 2014
Obamacare’s Enrollment Increase: Mainly Due to Medicaid Expansion
Health insurance enrollment data show that the number of Americans with private health insurance coverage increased by a bit less than 2.5 million in the first half of 2014. While enrollment in individual market coverage grew by almost 6.3 million, 61 percent of that gain was offset by a reduction of nearly 3.8 million individuals with employer-sponsored coverage. During the same period, Medicaid enrollment increased by almost 6.1 million—principally as a result of Obamacare expanding eligibility to able-bodied, working-age adults. Consequently, 71 percent of the combined increase in health insurance coverage during the first half of 2014 was attributable to 25 states and the District of Columbia adopting the Obamacare Medicaid expansion.
Adobe Acrobat document [159.5 KB]
October 20, 2014
Doc Fix Problems and Solutions
Medicare’s Sustainable Growth Rate (SGR) formula, put in place by the Balanced Budget act of 1997, was meant to control costs in Medicare by automatically reducing doctors’ pay. But without fail since 2003, Congress blocks SGR’s implementation each year. This is called a “doc fix.” The annual “doc fix” undermines the original purpose of the formula: to control Medicare costs. But allowing the SGR formula to take effect would lead to other problems. More than 50 million seniors depend on Medicare for health insurance. If physician reimbursement becomes too low, more and more doctors will close their doors to Medicare patients in favor of patients with private insurance. The government needs realistic, market-rate reimbursement policies to ensure that Medicare patients have access to the care they need.
Adobe Acrobat document [597.0 KB]
October 06, 2014
How Obamacare Is Affecting Wisconsin’s Workers and Employers
The Affordable Care Act contains sweeping changes to the employer-sponsored health insurance market. Though it was promoted as a way to lessen the problems small businesses experience in providing health coverage, many Wisconsin business owners report that the law is increasing their burden. Indeed, the Obama Administration itself says that perhaps two-thirds of small employers will see a jump in premiums due to provisions in the health care law. This trend is likely to continue.
Adobe Acrobat document [1.1 MB]
September 15, 2014
ObamaCare’s Impact on Small Business Wages and Employment
As the Federal Reserve found more than a decade ago, there is “strong evidence that workers pay for their health care costs in the form of reduced compensation, and that they do so contemporaneously with those costs.” Today, American Action Forum finds that the Affordable Care Act has fundamentally changed the health care landscape, affecting premiums, small business wages, and employment. $22.6 billion in foregone income and 350,000 lost small business jobs might sound like stark numbers, but they are just the initial data from the ACA’s implementation. We expect this trend to strengthen as the administration fully implements the employer mandate.
Adobe Acrobat document [392.4 KB]
Get in Touch With Me.
Call me at 405 810-8119 with any questions or to schedule an appointment.
Greg Karnes CPA
4301 NW 63rd St, Suite 200
Oklahoma City, OK 73116-1504
Or you may use my contact form.
Competitive Fee Structure
… but if you are looking for the cheapest fees, or obsessing about your correct pronouns or global warming/white privilege B.S., or unable to make up your mind as to whether you are a man or a woman, you would be so much happier working with someone else…
… in addition, due to an extremely hectic schedule, only serious inquiries may expect a response …
New tax clients are expected to provide copies of their last 3 years of tax returns and provide permission to contact prior accountant to resolve any issues, if necessary.
Regretfully, I am unable to accept new clients who have unfiled prior-year’s tax returns, who are not current with all prior tax obligations, are involved in any marijuana-related business ventures, use marijuana or illegal drugs, have any income from gambling, invest in cryptocurrency, are experiencing extreme financial difficulties, are personal-injury attorneys, in the construction industry or are in the country illegally. Newly formed businesses are frowned upon as well.
Though not required, supporters of President Donald J. Trump, Governor Kevin Stitt, the National Rifle Association & clients who are alpha males & females, ethical, hard-working, cheerful, optimistic and NOT easily offended are generally preferred.
Absolutely NO LAZY, TREE-HUGGING, CRITICAL RACE THEORY PROMOTING, ECONOMICALLY ILLITERATE, GODLESS, RIOTING, KNEELING, CENSORING, RACIALLY & GENDER OBSESSED, DR. SEUSS BOOK-BANNING, FIREARM CONFISCATING, BIG GOVERNMENT SOCIALISTS allowed beyond the front door, however!
Due to the alleged gang activity and drug dealing at the nearby Chelsea Manor Apts. & 7-11 Convenience Store, I would personally recommend "packing some heat" while in this area (and perhaps Penn Square Mall as well). Some believe the OKC Police Dept. has become too constrained and are hesitant to confront these gangbangers and put them behind bars where they rightfully belong. "Talk on the Street" seems to be that this emanates from an extremely weak & naive Mayor who purportedly suffers from a severe case of "Low T," a weak City Manager, a new, effeminate-looking Police Chief, who refuses to enforce our nation's immigration laws & a Ward 6 Council Girl who took her Oath Of Office using a book on Marxism.

Anyone that treats black Americans differently does so because @BarackObama has been saying that they are different for the last 10 years. The reality is, they are not and should not be. https://t.co/YxuH5rHjUW pic.twitter.com/0Et5yXEMl1
— Bernard B. Kerik (@BernardKerik) April 20, 2021
Everything that Mayor David “Pajama Boy” Holt & Police Chief “Wily” Wade Gourley need to know to improve law enforcement in OKC is in this book…if only they had some courage...

Calm Guide Sheet by Greg Karnes on Scribd
When you are hunting elephants, don’t get distracted chasing rabbits.
— T. Boone Pickens (@boonepickens) March 7, 2011

... coming from someone who should know! https://t.co/H2OwzJquyg via @TMZ_Sports
— Greg Karnes (@realGregKarnes) January 3, 2019



The duration of a mass shooting always depends on the arrival of the 2nd gun.
— longhorn_92 (@jaelvoet) December 30, 2019
And Democrats want to ban you from protecting yourself. Remember that next time you vote. pic.twitter.com/7N6GBPwYig
✅ An #ArmedCitizen saved multiple lives last night in #OKC. We hope this serves as a wake-up call for @GovMaryFallin, who just two weeks ago vetoed a constitutional carry bill. Just another example of how the best way to stop a bad guy with a gun is a good guy with a gun. #2A pic.twitter.com/kPRjpiyeow
— NRA (@NRA) May 25, 2018


Need to be a long-time Sooner football fan to appreciate.
— Greg Karnes (@realGregKarnes) February 22, 2020
Video taken 2 1/2 years ago in a friend's kitchen.
Former Sooner broadcaster John "Disco" Brooks & Marcus Dupree.
Also cameo by former Sooner/Sam Bradford's dad, Kent, & former Mayor Mick Cornett. pic.twitter.com/f5VZKxuvsm

Make The University of Oklahoma Great Again!
(Let us return to the time before the “Loudmouth Communist Snowflakes” and the less than competent financial administrators arrived on campus)
At the University of Oklahoma, the researchers found there were nearly nine registered Democrats for every one Republican on the faculty, and faculty gave $2 in campaign contributions to Democrats for every $1 given to Republicanshttps://t.co/l4Pzb3b5Q9
— Greg Karnes (@realGregKarnes) February 2, 2020
Citing Black Lives Matter, photos of retired white male professors to be taken down at U. Oklahoma
— Greg Karnes (@realGregKarnes) August 26, 2020
...I keep telling people that my alma mater has become a hotbed of Marxist thinking...
https://t.co/vutEDHcNpm
Are these ridiculous demands an inevitable consequence of my alma mater staffing the University with so many card-carrying Marxists?https://t.co/9LY2o7OsBr
— Greg Karnes (@realGregKarnes) August 10, 2020
Sadly, the University of Oklahoma is becoming a hotbed of Communist snowflakes.
— Greg Karnes (@realGregKarnes) September 27, 2019
Perhaps someday we can rebuild the University back to something that the football team can be proud of! https://t.co/Y0DrXXyUjN via @OUDaily
Looks to me some government employee violated the law. pic.twitter.com/5zOuXd8aei
— Mark Sharpton (@MarkSharpton) February 23, 2020
Pledge of Allegiance removed from OU undergraduate congressional agenda.
— Greg Karnes (@realGregKarnes) September 27, 2019
Student Philip Aldridge seems to have nailed it.https://t.co/DEtZId6xmP
Former OU volleyball player sues over exclusion from team because of Conservative political views
— Greg Karnes (@realGregKarnes) June 3, 2021
...my alma mater continues its trend towards forcing Marxist & radical views on the student body...hope she takes them to the cleanershttps://t.co/VSA5B60CZD
ODELL BECKHAM JR.
NOVEMBER 23, 2014
GREATEST CATCH EVER ??

RUSSELL WESTBROOK
FEBRUARY 16, 2015
NBA ALL STAR GAME MVP
41 POINTS
3RD MOST EVER SCORED

OU SOONER - SAMAJE PERINE
NOVEMBER 22, 2014
427 RUSHING YARDS
MOST EVER BY A COLLEGE RUNNING BACK

1/ Known for basketball prowess, Wayman Tisdale's 'further legacy is his love of God'
— Greg Karnes (@realGregKarnes) April 10, 2021
...saw this story in today's paper regarding Wayman Tisdale and couldn't help but be reminded of Toby Keith's tribute song to his friend...https://t.co/4RiPYofGB7
Top 10
Taxpayer Enemies
Those Individuals Or Groups Who Seem Most Intent On Penalizing Success & Achievement & Desiring A Return To The Days Of Low Economic Growth During The Jimmy Carter/Barry Obama - "Sleepy Joe" Biden Era
(in order, as of today)

“Since this is an era when many people are concerned about ‘fairness’ and ‘social justice,’ what is your ‘fair share’ of what someone else has worked for?”
— Thomas Sowell (@ThomasSowell) January 8, 2019







The Caracas Caucus
(the Top 10 “Americans” who seem most hell-bent on destroying our jobs & economy in order to advance the cause of centralized government control over our lives and private businesses to the point where we are forced to surrender our individual liberties to the state)
— Greg Karnes (@realGregKarnes) March 29, 2021




The Terrorist Caucus
Those Individuals Or Groups Who
Come Across To Me As Ambivalent Towards Islamic
Terror Activities





The "Soft On Crime"
"Hug-A-Thug" Caucus
The Top 10 Individuals Or Groups Who
Come Across To Me As Coddling The Criminal Element At The Expense Of The Public Safety Of Law-Abiding Citizens






The “Ugly” Caucus
The Top 10 Individuals On The Taxpayer Payroll That Strike Me As Being Just As Unattractive On The Inside As They Are On The Outside.


LOWER TAXES
=
HIGHER GOVERNMENT REVENUE



This should be simple enough for everyone to understand. pic.twitter.com/tWsu50ewvL
— Juanita Broaddrick (@atensnut) October 21, 2021
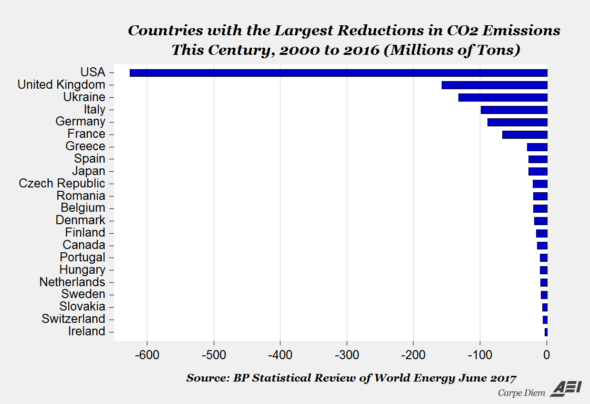
The United States leads the world in CO2 reductions

Is the individual depicted above the most ill-prepared person Oklahoma has ever had in a General Election for a U.S. Senate seat?
