
May 27, 2017
America cannot sustainably add 77 million retiring baby boomers to a Medicare system that collects $140,000 in lifetime taxes from the typical retiring couple and then provides them with $422,000 in benefits (all adjusted into net present values) without slashing other programs to the bone. […]
September 11, 2015
A Simple Change to Restore Social Security Solvency (From Tax Foundation - Stephen J. Entin)
We have paid a stiff penalty by waiting nearly 40 years to adopt price indexing. The baby boomers have begun to retire, and the Old Age and Survivors Insurance system is already in deficit. Nonetheless, the projected OASI deficits would be brought down to a manageable size with price indexing. Without price indexing or some other trimming of the growth of benefits, there can be no permanent fix to the program without substantial loss of jobs and income.
April 15, 2015
Expansion of Medicaid at the Expense of Our Future: Proposed Reforms Critical to Improve Long-Term Access to Affordable, Quality Care
Since 2010, the federal government has been attempting to entice, cajole, and even coerce Florida and other states to expand Medicaid in accordance with the rollout of Obamacare. When a large portion of a hospital’s patients cannot afford to pay, those hospitals turn to the taxpayers for help, often in the form of the Low Income Pool (LIP) Program. Now the Obama administration has announced it intends to cut off this aid because Florida has not expanded eligibility for Medicaid. By playing politics with Florida’s LIP funding, the administration is showing a blatant disregard for the hospitals that serve low-income residents and a contempt of the Constitution. There is no reason to believe that expanding the Medicaid program would increase access to quality care. Florida’s leaders should focus on the long-term and being to implement reasonable, sound reforms that will first and foremost have a positive impact on our strained healthcare system.
April 13, 2015
Fix the Flawed Medicare Doc Fix
For over a decade, Congress has struggled with an inadequate formula to calculate Medicare payments to physicians. The formula results in an amount too low to ensure physicians will continue to see Medicare beneficiaries. At least once a year, Congress has to pass a short-term increase to Medicare physician payments to prevent fees dropping about 20 percent. The current boost expired on March 31, 2015, necessitating a rapid response. Three options are available to reduce the shortcomings of the Medicare Access and CHIP Reauthorization Act (MACRA) and keep the door open to effective Medicare reform: 1. A two-year doc fix, paralleling the extension of the Children’s Health Insurance Plan in MACRA. 2. Including MACRA in the pay-as-you-go scorecards, requiring the president to pay for it with other funds. 3. Finding offsets to pay for the $141 billion in MACRA spending that is not yet offset.
March 23, 2015
Replacing Medicare’s Unsustainable Sustainable Growth Rate
We propose setting Medicare reimbursement rates through comparison with the closest available approximation of actual market prices for health care, those experienced by patients enrolled in the substantial and growing Medicare Advantage (MA) program. In this proposal, MA, which permits those 65 and older to choose from among a group of private insurance plans, would serve as a source of benchmark pricing for so-called Medicare fee-for-service patients—the majority of Medicare enrollees whose health care providers are reimbursed, at a predetermined price, for each individual service performed. The plan offered herein combines the potential for predictability—of the sort health care providers much prefer—with the potential for cost controls originally envisioned by the Sustainable Growth Rate approach.
Adobe Acrobat document [108.6 KB]
March 20, 2015
Medicaid Expansion: A Lesson in Unreliability
As Florida debates ways to improve care for the uninsured and underinsured, it is very important to grasp the problems that currently plague the Medicaid program. These flaws are not mere peripheral trivialities. Rather, they are deeply rooted at the core of the Medicaid statute. They cannot be rectified without comprehensive Medicaid reform, and they are too grave a burden to impose on more people.
Adobe Acrobat document [97.8 KB]
February 25,2015
Raising the tax cap wouldn’t even make Social Security solvent anyway. (From National Review – Andrew Biggs)
February 05, 2015
Three Medicaid Expansion Myths Exposed
The “Texas Solution” would simply be the Obamacare Medicaid expansion by another name, just as it has been in every state that has tried and failed to gain flexibility from the federal government. If Texas does not expand Medicaid, our tax dollars do not go to other states; the federal government will simply spend less on Medicaid. The final myth is exposed because expanding Medicaid would only cover an estimated 13 percent of the state’s uninsured population in 2015, leaving millions still uninsured.
Adobe Acrobat document [113.6 KB]
December 11, 2014
Previous studies predict large and beneficial macroeconomic effects of the ACA's Medicaid expansion, by calculating the economic benefits to individual states of the inflow of federal dollars predicted to ensue. However, in calculating those benefits, these studies typically ignore one or more offsetting factors, most notably the taxes necessary to pay for the Medicaid expansion, the deadweight loss associated with this taxation, and even the direct loss of premium subsidies that accompany eligibility for Medicaid.
When we take these offsetting factors into account, the picture changes considerably. Instead of an increase in economic growth and jobs, we find the opposite occurs—billions of dollars of economic activity, and thousands of jobs, are lost. Some states see small net gains, but the total losses incurred in other states substantially exceed the total gains.
Adobe Acrobat document [378.0 KB]
Adobe Acrobat document [226.5 KB]
November 26, 2014
Medicare and the Free Market
Allowing balance billing for Medicaid patients would price many Medicaid doctors back into the system. One worry is that doctors would charge very high prices to Medicaid patients, well above what they are allowed to charge now. But this seems unlikely. The reason is simple: poor and near-poor people can’t afford to pay much, and so doctors who consistently charged, say, 50 percent more than Medicaid pays would likely find few takers. But there’s a simple solution that’s similar to my in-between proposal for Medicare: limit the balance billing to, say, a 10-percent mark-up over the Medicaid fee. This would give a little added incentive to doctors to service people on Medicaid and a potentially large incentive for people on Medicaid to pay attention to prices in their decisions.
Adobe Acrobat document [950.6 KB]
November 18, 2014
How Two States Cut Medicaid and Saved Money
While Pennsylvania focused on its broader welfare population, Illinois directed its redetermination efforts primarily at the Medicaid program. Both efforts succeeded, though the Illinois redetermination program received bipartisan support, while there were numerous critics of the Pennsylvania effort. States are facing serious Medicaid budget challenges and many need to address the problem quickly. A redetermination program is a good start. Fighting waste and fraud can be a bipartisan battle. Getting ineligible beneficiaries off the rolls allows the state to use that money for other purposes—or return it to the taxpayers.
Adobe Acrobat document [131.6 KB]
November 07, 2014
Understanding the CBO’s Change in Medicare Spending Projections
The Congressional Budget Office (CBO) has lowered its projections for Medicare spending over the next decade. A variety of factors are contributing to the reduced projections, some of which are unlikely to be sustained due to their negative impact on beneficiaries. Regardless, the decreased projections do not reduce the need for Medicare reform. The CBO still projects total Medicare spending—and spending in each subprogram part—to increase steadily, surpassing $1 trillion annually by 2023. Thus, the slowdowns in annual spending projections say nothing about the program’s long-term fiscal health. Medicare’s current structure remains unsustainable and in desperate need of structural reform.
Adobe Acrobat document [446.8 KB]
November 06, 2014
Medicare Drug Plans Need the Tools to Fight Prescription Drug Fraud
In August 2014, the Office of the Inspector General within the U.S. Department of Health and Human Services issued recommendations to reduce questionable drug use by Medicare beneficiaries. Such a program is currently being debated in Congress. In August 2014, the Chairman of the House Ways and Means Subcommittee on Health, Kevin Brady (R-Texas), circulated a draft of a bill designed to help Medicare drug plans reduce fraud. The “Protecting Integrity in Medicare Act of 2014” would give drug plans within Medicare Part D the authority to restrict certain beneficiaries to the use of a single doctor and pharmacy with respect to specific opioids and other high-risk drugs. Drug plans are currently hamstrung by regulations that prevent them from tackling drug abuse, and they need this type of flexibility in order to effectively combat fraud.
Adobe Acrobat document [1.1 MB]
August 04, 2014
Social Security Trustees Report: Unfunded Liability Increased $1.1 Trillion and Projected Insolvency in 2033
Social Security ran a $71 billion deficit in 2013, closing out four years of consecutive cash-flow deficits as the program’s unfunded obligations continue to grow. Despite being solvent for about two more decades, the Social Security and Disability Insurance programs are already contributing to annual deficits. Absent reform, Social Security benefits will be cut across the board by 23 percent in 2033. Action should be taken today to protect Social Security’s most vulnerable beneficiaries from such drastic cuts without burdening younger generations through tax increases. Lawmakers should immediately replace the current cost-of-living adjustment with the more accurate chained Consumer Price Index, raise the early and full retirement ages gradually and predictably, focus Social Security benefits on those who need them most, and alleviate poverty in old age with a minimum flat benefit.
Adobe Acrobat document [231.2 KB]
July 31, 2014
The Mechanics of Medicaid
The flaws in our half-billion-dollar Medicaid program stem from the way in which it is funded, as both state and federal government share the bill. North Carolina’s $14 billion Medicaid program currently pulls down a 65 percent federal match — well above the national average. Federal funding creates a strong disincentive for North Carolina to flush out waste in the system, since a hefty portion of any savings reverts back to the feds. The state could use excess federal funds for budget purposes not limited to Medicaid. If Medicaid’s federal share was transferred to North Carolina as an annual block grant, the state would have to shoulder more program costs. But such an injection of fiscal responsibility would allow lawmakers to exercise more control over the program and create a stronger incentive to sort out system waste and abuse.
Adobe Acrobat document [302.8 KB]
July 31, 2014
The Future of America’s Entitlements: What You Need to Know About the Medicare Trustees Report
Medicare and Social Security are (still) going bankrupt. At its current pace, Medicare will be bankrupt in 2030, and Social Security will go bankrupt in 2033. Medicare is the principal driver of the United States debt. With Medicare facing unprecedented levels of cash shortfalls, Medicare Advantage benefits facing significant cut, and 14 million Americans facing the loss of their Part D plans, it’s evident that President Obama and the Affordable Care Act have failed to ensure that Medicare will be there for today’s seniors, let alone the next generation of older Americans. Projections for Social Security and Disability Insurance are equally grim. Without substantial reform, these programs will be bankrupt in less than two decades, and Americans will be chained to a debt many times the size of the debt that we face now.
Adobe Acrobat document [153.5 KB]
Washington will never gain control of federal budget deficits unless it clearly identifies their underlying causes. The vast majority—more than three-fourths—of the currently projected long-term fiscal imbalance derives from a set of decisions made between 1965 and 1972: specifically, the creation and subsequent expansion of Medicare and Medicaid and the automatic indexation of Social Security benefits. The current-year deficit exists largely because of growth in Social Security, Medicare and Medicaid spending, in combination with recent expansions of income security programs and lower-than-typical revenue collections.
Federal Budget Deficits.pdf
Adobe Acrobat document [345.5 KB]
December 19, 2013
How Competition Drives Savings in Medicare Part D
Part D and Medicare Advantage plans represent the first national health-care exchange (the Federal Employees’ Health Benefits Program [FEHBP] is a close cousin). While the Affordable Care Act (ACA) operates a similar exchange concept, there are important differences. First, Part D plans compete in large regional areas, not states (this creates much bigger risk pools because even large states are incorporated into larger regions), as the ACA exchanges do. Even the federal exchange is layered on top of a state-regulated insurance market. This potentially limits the ability of plans to create economies of scale to bargain with providers and to utilize innovative tools to arbitrage cost and quality differences across state markets (preferred pharmacy and mail-order networks in Part D; telemedicine and medical tourism to “centers of excellence” for health-insurance plans).
How Competition Drives Savings in Medica[...]
Adobe Acrobat document [1.5 MB]
Get in Touch With Me.
Call me at 405 810-8119 with any questions or to schedule an appointment.
Greg Karnes CPA
4301 NW 63rd St, Suite 200
Oklahoma City, OK 73116-1504
Or you may use my contact form.
Competitive Fee Structure
… but if you are looking for the cheapest fees, or obsessing about your correct pronouns or global warming/white privilege B.S., or unable to make up your mind as to whether you are a man or a woman, you would be so much happier working with someone else…
… in addition, due to an extremely hectic schedule, only serious inquiries may expect a response …
New tax clients are expected to provide copies of their last 3 years of tax returns and provide permission to contact prior accountant to resolve any issues, if necessary.
Regretfully, I am unable to accept new clients who have unfiled prior-year’s tax returns, who are not current with all prior tax obligations, are involved in any marijuana-related business ventures, use marijuana or illegal drugs, have any income from gambling, invest in cryptocurrency, are experiencing extreme financial difficulties, are personal-injury attorneys, in the construction industry or are in the country illegally. Newly formed businesses are frowned upon as well.
Though not required, supporters of President Donald J. Trump, Governor Kevin Stitt, the National Rifle Association & clients who are alpha males & females, ethical, hard-working, cheerful, optimistic and NOT easily offended are generally preferred.
Absolutely NO LAZY, TREE-HUGGING, CRITICAL RACE THEORY PROMOTING, ECONOMICALLY ILLITERATE, GODLESS, RIOTING, KNEELING, CENSORING, RACIALLY & GENDER OBSESSED, DR. SEUSS BOOK-BANNING, FIREARM CONFISCATING, BIG GOVERNMENT SOCIALISTS allowed beyond the front door, however!
Due to the alleged gang activity and drug dealing at the nearby Chelsea Manor Apts. & 7-11 Convenience Store, I would personally recommend "packing some heat" while in this area (and perhaps Penn Square Mall as well). Some believe the OKC Police Dept. has become too constrained and are hesitant to confront these gangbangers and put them behind bars where they rightfully belong. "Talk on the Street" seems to be that this emanates from an extremely weak & naive Mayor who purportedly suffers from a severe case of "Low T," a weak City Manager, a new, effeminate-looking Police Chief, who refuses to enforce our nation's immigration laws & a Ward 6 Council Girl who took her Oath Of Office using a book on Marxism.

Anyone that treats black Americans differently does so because @BarackObama has been saying that they are different for the last 10 years. The reality is, they are not and should not be. https://t.co/YxuH5rHjUW pic.twitter.com/0Et5yXEMl1
— Bernard B. Kerik (@BernardKerik) April 20, 2021
Everything that Mayor David “Pajama Boy” Holt & Police Chief “Wily” Wade Gourley need to know to improve law enforcement in OKC is in this book…if only they had some courage...

Calm Guide Sheet by Greg Karnes on Scribd
When you are hunting elephants, don’t get distracted chasing rabbits.
— T. Boone Pickens (@boonepickens) March 7, 2011

... coming from someone who should know! https://t.co/H2OwzJquyg via @TMZ_Sports
— Greg Karnes (@realGregKarnes) January 3, 2019



The duration of a mass shooting always depends on the arrival of the 2nd gun.
— longhorn_92 (@jaelvoet) December 30, 2019
And Democrats want to ban you from protecting yourself. Remember that next time you vote. pic.twitter.com/7N6GBPwYig
✅ An #ArmedCitizen saved multiple lives last night in #OKC. We hope this serves as a wake-up call for @GovMaryFallin, who just two weeks ago vetoed a constitutional carry bill. Just another example of how the best way to stop a bad guy with a gun is a good guy with a gun. #2A pic.twitter.com/kPRjpiyeow
— NRA (@NRA) May 25, 2018


Need to be a long-time Sooner football fan to appreciate.
— Greg Karnes (@realGregKarnes) February 22, 2020
Video taken 2 1/2 years ago in a friend's kitchen.
Former Sooner broadcaster John "Disco" Brooks & Marcus Dupree.
Also cameo by former Sooner/Sam Bradford's dad, Kent, & former Mayor Mick Cornett. pic.twitter.com/f5VZKxuvsm

Make The University of Oklahoma Great Again!
(Let us return to the time before the “Loudmouth Communist Snowflakes” and the less than competent financial administrators arrived on campus)
At the University of Oklahoma, the researchers found there were nearly nine registered Democrats for every one Republican on the faculty, and faculty gave $2 in campaign contributions to Democrats for every $1 given to Republicanshttps://t.co/l4Pzb3b5Q9
— Greg Karnes (@realGregKarnes) February 2, 2020
Citing Black Lives Matter, photos of retired white male professors to be taken down at U. Oklahoma
— Greg Karnes (@realGregKarnes) August 26, 2020
...I keep telling people that my alma mater has become a hotbed of Marxist thinking...
https://t.co/vutEDHcNpm
Are these ridiculous demands an inevitable consequence of my alma mater staffing the University with so many card-carrying Marxists?https://t.co/9LY2o7OsBr
— Greg Karnes (@realGregKarnes) August 10, 2020
Sadly, the University of Oklahoma is becoming a hotbed of Communist snowflakes.
— Greg Karnes (@realGregKarnes) September 27, 2019
Perhaps someday we can rebuild the University back to something that the football team can be proud of! https://t.co/Y0DrXXyUjN via @OUDaily
Looks to me some government employee violated the law. pic.twitter.com/5zOuXd8aei
— Mark Sharpton (@MarkSharpton) February 23, 2020
Pledge of Allegiance removed from OU undergraduate congressional agenda.
— Greg Karnes (@realGregKarnes) September 27, 2019
Student Philip Aldridge seems to have nailed it.https://t.co/DEtZId6xmP
Former OU volleyball player sues over exclusion from team because of Conservative political views
— Greg Karnes (@realGregKarnes) June 3, 2021
...my alma mater continues its trend towards forcing Marxist & radical views on the student body...hope she takes them to the cleanershttps://t.co/VSA5B60CZD
ODELL BECKHAM JR.
NOVEMBER 23, 2014
GREATEST CATCH EVER ??

RUSSELL WESTBROOK
FEBRUARY 16, 2015
NBA ALL STAR GAME MVP
41 POINTS
3RD MOST EVER SCORED

OU SOONER - SAMAJE PERINE
NOVEMBER 22, 2014
427 RUSHING YARDS
MOST EVER BY A COLLEGE RUNNING BACK

1/ Known for basketball prowess, Wayman Tisdale's 'further legacy is his love of God'
— Greg Karnes (@realGregKarnes) April 10, 2021
...saw this story in today's paper regarding Wayman Tisdale and couldn't help but be reminded of Toby Keith's tribute song to his friend...https://t.co/4RiPYofGB7
Top 10
Taxpayer Enemies
Those Individuals Or Groups Who Seem Most Intent On Penalizing Success & Achievement & Desiring A Return To The Days Of Low Economic Growth During The Jimmy Carter/Barry Obama - "Sleepy Joe" Biden Era
(in order, as of today)

“Since this is an era when many people are concerned about ‘fairness’ and ‘social justice,’ what is your ‘fair share’ of what someone else has worked for?”
— Thomas Sowell (@ThomasSowell) January 8, 2019







The Caracas Caucus
(the Top 10 “Americans” who seem most hell-bent on destroying our jobs & economy in order to advance the cause of centralized government control over our lives and private businesses to the point where we are forced to surrender our individual liberties to the state)
— Greg Karnes (@realGregKarnes) March 29, 2021




The Terrorist Caucus
Those Individuals Or Groups Who
Come Across To Me As Ambivalent Towards Islamic
Terror Activities





The "Soft On Crime"
"Hug-A-Thug" Caucus
The Top 10 Individuals Or Groups Who
Come Across To Me As Coddling The Criminal Element At The Expense Of The Public Safety Of Law-Abiding Citizens






The “Ugly” Caucus
The Top 10 Individuals On The Taxpayer Payroll That Strike Me As Being Just As Unattractive On The Inside As They Are On The Outside.


LOWER TAXES
=
HIGHER GOVERNMENT REVENUE



This should be simple enough for everyone to understand. pic.twitter.com/tWsu50ewvL
— Juanita Broaddrick (@atensnut) October 21, 2021
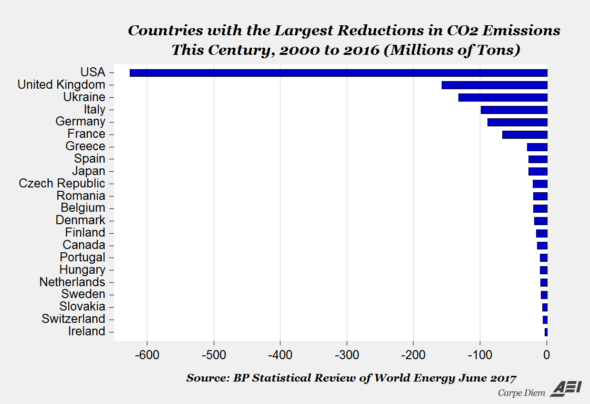
The United States leads the world in CO2 reductions

Is the individual depicted above the most ill-prepared person Oklahoma has ever had in a General Election for a U.S. Senate seat?
